
Reverse Shoulder Replacement in San Antonio, TX
What Is Reverse Shoulder Replacement?
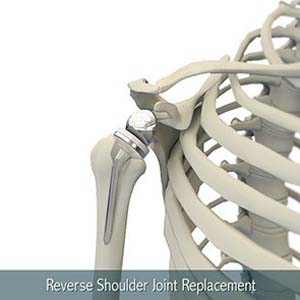
Reverse total shoulder replacement is an engineered solution to a specific problem: a shoulder that has both arthritis and a severely compromised rotator cuff, or in shoulder with significant wear that does not allow for conventional shoulder replacement. In an anatomic (conventional) shoulder replacement the rotator cuff muscles are responsible for stabilizing and moving the prosthetic joint. When the cuff is irreparably torn or absent, that system fails and an anatomic replacement becomes painful and unstable.
The reverse arthroplasty solves this by switching the positions of the ball and socket. The metal ball is fixed to the glenoid (shoulder blade socket) and the plastic cup receives the top of the humerus. This geometric reversal shifts the center of rotation and puts the deltoid muscle, which remains functional even when the rotator cuff is gone, in a mechanical position where it can power shoulder elevation without cuff assistance.
The result for appropriately selected patients is reliable pain relief and functional arm elevation that was often impossible before surgery.
Who Is a Candidate?
Reverse shoulder replacement is the procedure of choice for:
- Rotator cuff tear arthropathy — the combination of end-stage arthritis and a massive, irreparable cuff tear
- Massive rotator cuff tears with pseudoparalysis (inability to elevate the arm) even without advanced arthritis, in selected cases
- Failed prior anatomic shoulder replacement where the rotator cuff has subsequently failed
- Complex proximal humerus fractures in older patients where reconstruction is not feasible
- Revision cases following failed prior shoulder arthroplasty
Reverse replacement is increasingly used in younger, more active patients with the right anatomy and indication, not just elderly patients. The decision requires careful analysis of bone quality, remaining muscle function, prior surgical history and realistic activity goals.
My Approach to Complex and Revision Cases
I have a particular interest in revision shoulder arthroplasty; cases where a prior replacement has failed due to instability, component loosening, infection or periprosthetic fracture. These cases require advanced preoperative planning, often including CT-based bone stock assessment and custom or augmented implant systems. Not every surgeon who performs primary shoulder replacement is experienced in the revision setting, and I am candid with patients when a case complexity warrants that conversation.
For primary reverse arthroplasty, I use CT-based preoperative planning to optimize baseplate positioning on the glenoid, the most critical technical determinant of long-term implant survival. Errors in glenoid version and inclination that are acceptable in anatomic arthroplasty become magnified in the reverse construct. Precision at the time of surgery is not optional.
What to Expect During Recovery
- Weeks 1 to 3: Sling, pendulum exercises and passive elevation began within the first week
- Weeks 4 to 8: Active range of motion, progressive functional activities
- Months 2 to 4: Strengthening, return to most daily activities
- Months 4 to 6: Activity-specific progression, recreational use for most patients
- Motion and strength may continue to improve up to 2 years after this surgery.
Patients who had limited arm elevation before surgery often notice functional improvement sooner than total shoulder replacement patients because the reverse construct immediately offloads the failed rotator cuff. Many of my reverse replacement patients are cooking, dressing and sleeping comfortably within the first month.
A Note on Expectations
Reverse shoulder replacement reliably addresses pain and restores forward elevation. External rotation recovery is variable and depends on the condition of the remaining rotator cuff muscles; specifically the teres minor. I discuss realistic, individualized expectations with every patient before surgery so the outcome conversation is honest rather than optimistic.
Why Choose Dr. Lynch
Reverse shoulder arthroplasty is the most technically demanding procedure in my specialty. Outcomes are directly tied to patient selection, implant positioning and surgical experience. I perform this procedure regularly as part of a dedicated shoulder arthroplasty practice, including complex revision cases and failed prior implants. I use patient-specific CT planning on every case. If you have been told your shoulder is not repairable or that you are not a surgical candidate, I encourage a second opinion; the complexity that makes one surgeon hesitant is often the situation I find most interesting.
Private-pay and commercial insurance patients welcome.
Ready to take the next step? Call (210) 878-4113 or request an appointment at sportssurgeryspecialist.com.
Quick Links
- Shoulder Anatomy
- Arthritis of the Shoulder
- Rotator Cuff Tear
- Shoulder Dislocation
- Frozen Shoulder
- Shoulder Instability
- Shoulder Fracture
- Biceps Tendon Rupture
- Shoulder Arthroscopy
- Total Shoulder Replacement
- Reverse Shoulder Replacement
- Shoulder Hemiarthroplasty
- Rotator Cuff Repair
- Shoulder Stabilization



